Potential drug targets on potassium and chloride channels
by egpat 30-09-2017
All our physiological functions depend on the action potentials which are rapidly communicated throughout our body activating various cells where ion channels are playing a key role in producing rapid and effective cellular response. Once this action potential reaches to the cell, the cell is activated by depolarisation of the membrane. This depolarisation is mediated by inward-going ion channels like sodium and calcium. The depolarisation phase is followed by a repolarisation phase mediated by outward-going ion channels like potassium. Few of the ion channels like chloride channels are inward going but inhibitory in nature preventing depolarisation. Hence all these ion channels act as great targets for many of the clinically important drugs.
In the previous article, we have discussed clinically important drugs acting on sodium and calcium channels. Now here we will discuss other drugs acting on potassium and chloride channels.
Voltage gated potassium channels
Voltage gated potassium channels are widely present in many of the cells responsible for repolarisation following a depolarisation phase. These channels are very important to bring the membrane potential back to resting state. One of the main target locations where clinically important drugs are acting is potassium channels on heart.
At heart, potassium channel are involved in both phase II and phase III.
In phase II, also called as plateau phase, the membrane potential remains constant as both potassium and calcium channels are opened and each transported in opposite directions to make the membrane potential constant. Phase II is not a good drug target for potassium channel blockers as potassium current is low and sufficient to counteract calcium current.
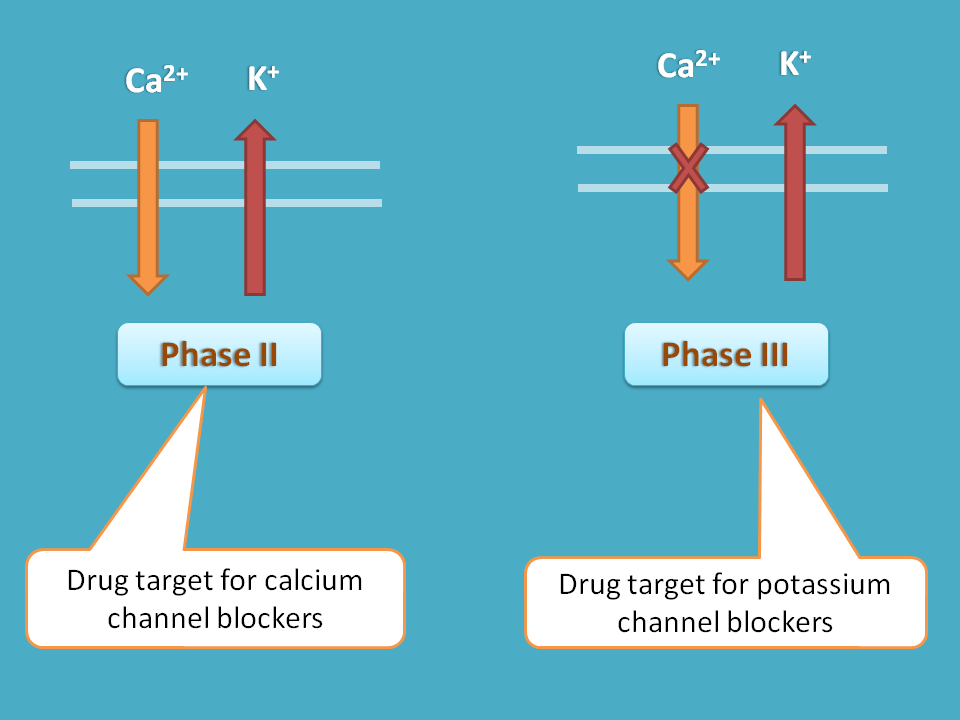
But in phase III, only potassium channels are acting and calcium channels are closed. This leads to complete repolarisation of the membrane bringing back the potential nearer to the resting membrane potential. Hence phase III acts as good drug target and one of the well known class III antiarrhythmic agents act on this phase.
Drugs included in this category are
- Amiodaranone
- Sotalol
- Dronedarone
- Mexiletine
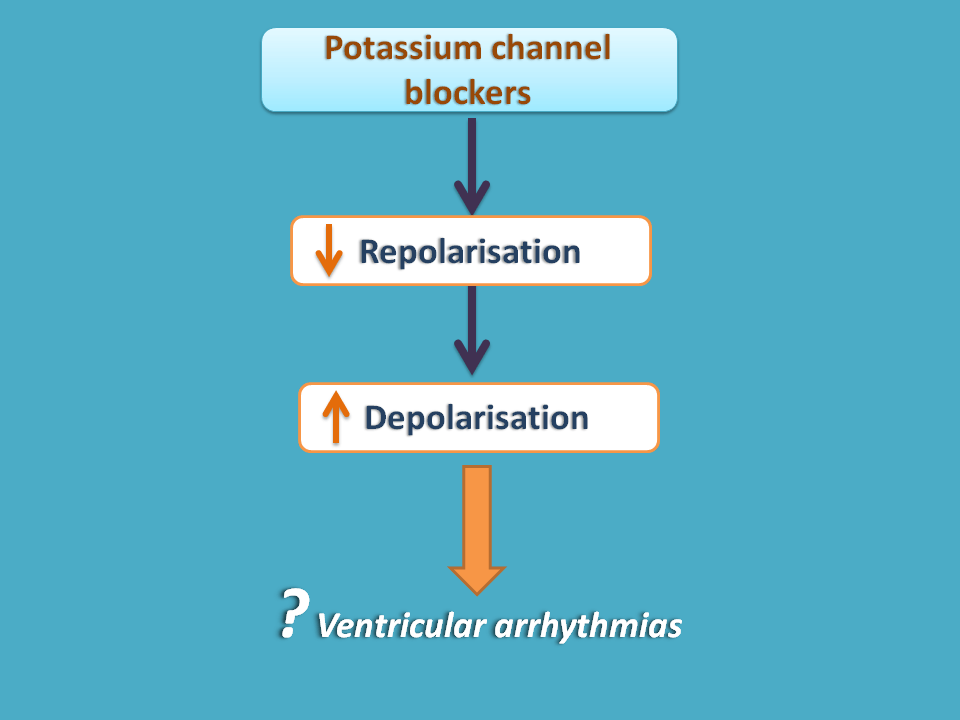
They effect repolarisation not depolarisation.
Cardiac arrhythmias, particularly those with increased heart rate are due to increased depolarisation of cardiac cells. So any drug acting on these should inhibit depolarisation. In contrast potassium channel blockers inhibit repolarisation which may increase cardiac arrhythmias. Then how they can be used in cardiac arrhythmias?
Yes, its true that cardiac arrhythmias like ventricular tachycardia are due to excess depolarisation of cardiac cells so any drug that inhibits this depolarisation are useful in this condition. For example, sodium channel blockers like lidocaine can be used in ventricular tachycardia.
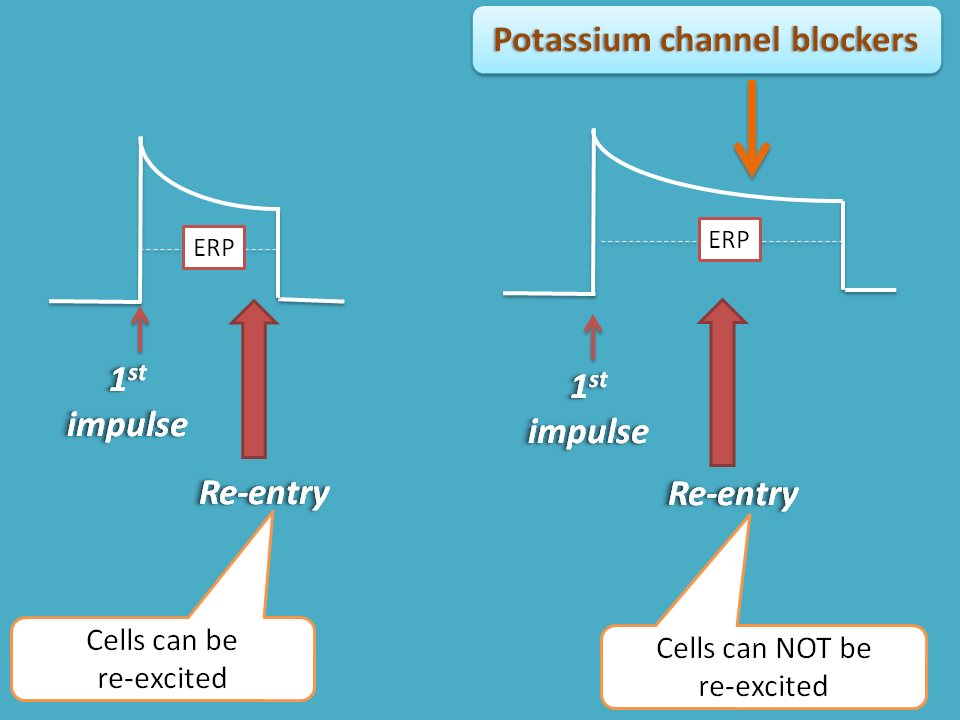
But we can also find few of re-entry type of arrhythmias where the cardiac cells are re-excited due to any conductional block where the effective of refractory period should be increased. Since potassium channel blockers inhibit repolarisation of cardiac cells, they produce widening of plateau phase so that net effective refractory period increases. So any extra beat within the timescale of this refractory period can be prevented.
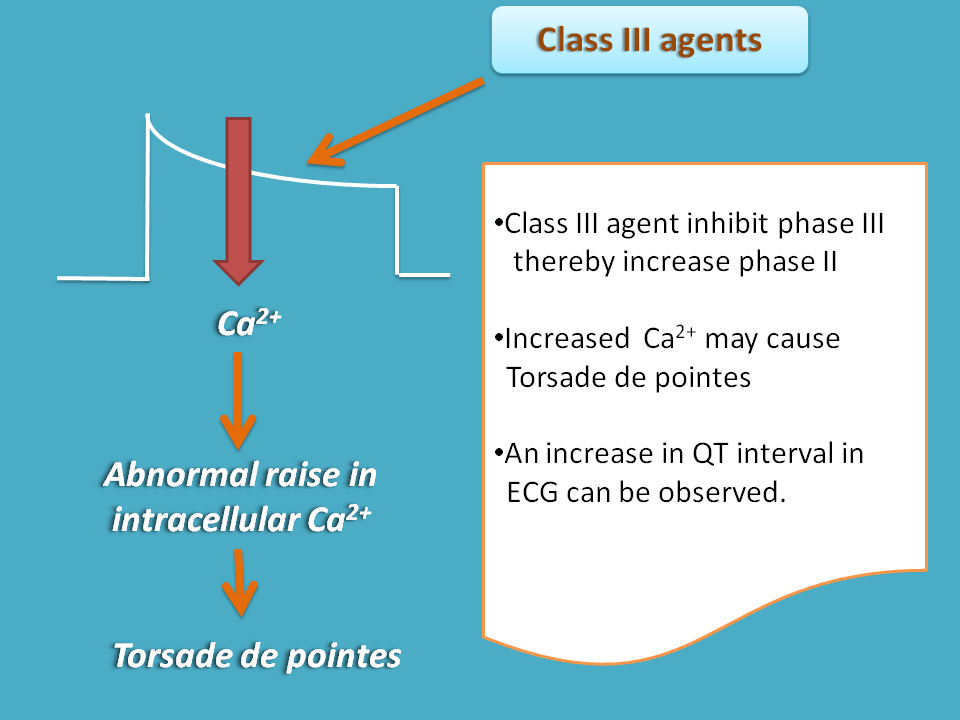
As these drugs enhance depolarisation at plateau phase, they may increase intracellular calcium levels within the heart increasing the risk of other types of ventricular arrhythmias. One such potential and life threatening arrhythmia, torsade de pointes , can be observed with these drugs.
That’s why these drugs are called as proarrhythmic.
Class III drugs suppress re-entry type of arrhythmia but can enhance other types of arrhythmias.
❞Amiodarone is an exceptional agent that blocks sodium and calcium channels in addition to potassium channels. It also blocks beta receptors. Therefore it shows all class actions of antiarrhythmic agents.
Side effects
As we have discussed earlier, one of the main concern of potassium channel blockers is torsade de pointes. Of course, this is not observed at normal dose but any other factors may enhance the risk. For example, drugs like chlorpromazine and haloperidol when given along with these drugs may precipitate torsade de pointes.
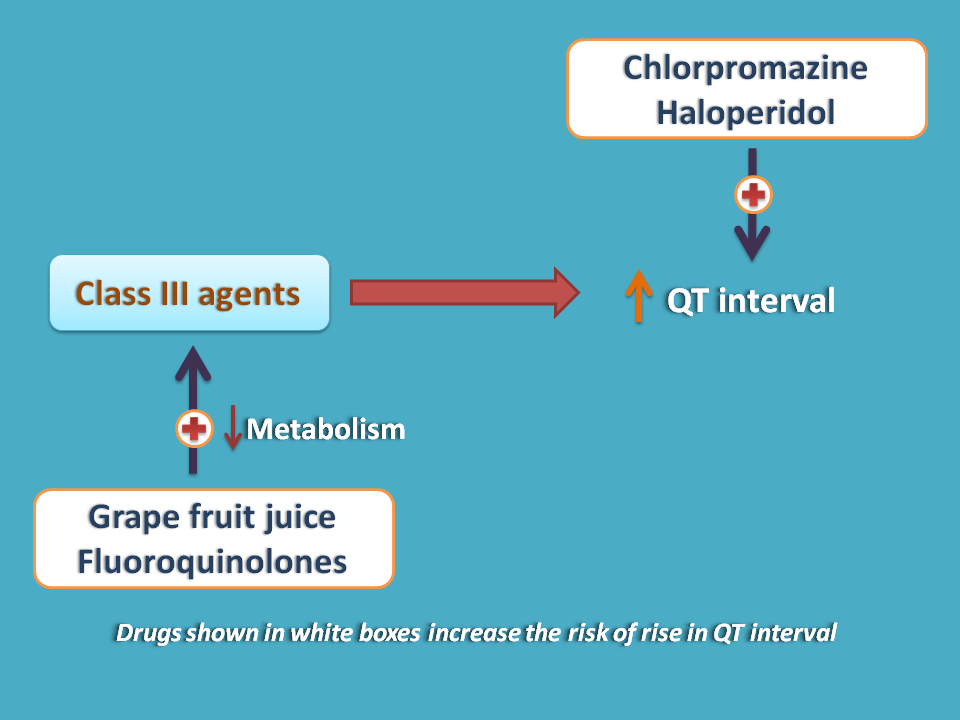
Sometimes food like grape fruit may juice may also interact with these drugs increasing the risk.
Amiodaraone also produces pulmonary fibrosis, corneal deposits and thyroid abnormalities such as hypo or hyperthyroidism.
- See here to know how amiodarone produce thyroid problems.
ATP sensitive potassium channels
Few of the specialised potassium channels are present on many of the cells including vascular smooth muscle and pancreatic beta cells. When these channels are opened they increase outflux of potassium leading to hyperpolarisation of the membrane. Two classes of drugs act on these ATP sensitive potassium channels.
- ATP sensitive potassium channel activators
- ATP sensitive potassium channel blockers
As we know that potassium is outward going and calcium is inward going. So potassium leads to repolarisation and calcium depolarisation.
ATP sensitive potassium channel activators
Since potassium channels are outward going, under normal conditions they can be activated to produce hyperpolarisation. This hyperpolarised membrane can’t be activated by either action potential or chemical mediator hence inhibited.
For example, ATP sensitive potassium channels are excessively opened in vascular smooth muscle by potassium channel openers where the membrane potential is too negative so that they can’t respond to any stimulus such as neurotransmitter or chemical mediator. It can’t undergo contraction as voltage gated L-type calcium channels are closed at this potential. This inhibition of vascular smooth muscle leads vasodilation.
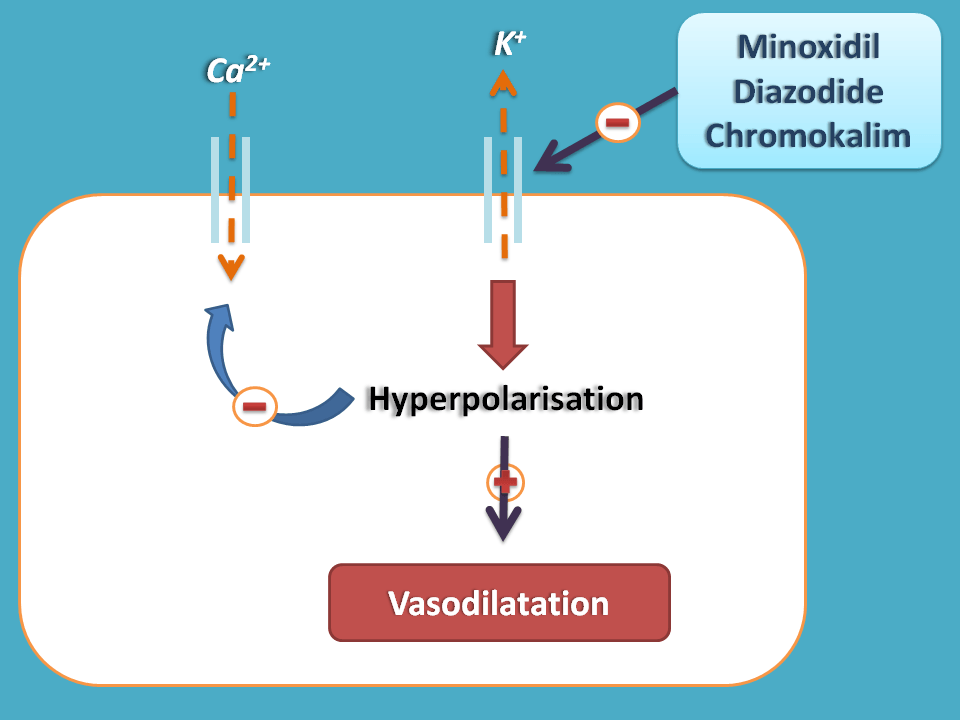
Minoxidil and diazoxide are such drugs that open ATP sensitive potassium channels on vascular smooth muscle and produce vasodilatation. Chromokalim is another drug that also acts as vasodilator. These drugs can be used in treatment of hypertension. Particularly minoxidil is used in severe hypertension.
Minoxidil can cause enhanced hair growth at face and other location which is unwanted. For the same reason, it can be used purposefully by topical route for treating baldness.
Nicorandil has unique property of dilation of both arteries and veins. It opens ATP sensitive potassium channels on vascular smooth muscle leading to hyperpolarisation.
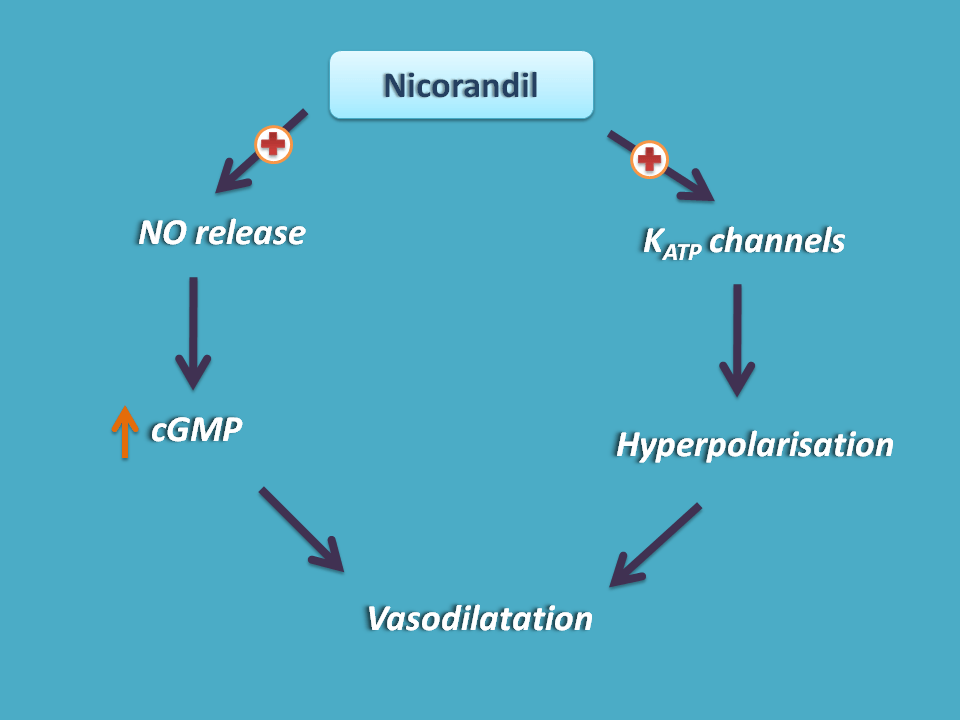
Structurally it has a nitrate group which can release nitric oxide. This released nitric oxide then increases cGMP levels in vascular smooth muscle leading to relaxation. Nicorandil can be used in the treatment of angina.
ATP sensitive potassium channel blockers
Which controls blood glucose levels?
Insulin is one of the hormone that controls blood glucose levels in two phases viz. basal phase and postprandial phase. Basal phase release of insulin is a continuous release of insulin at very low levels to just check the glucose levels in the blood throughout the day. On the otherhand, postprandial insulin release after a meal is very important to control sudden rise of glucose in the blood.
Release of insulin
So the main stimulus for the release of insulin is elevated blood glucose levels. This is generally observed after meal stimulating the release of insulin. But glucose is not directly involved instead the release is mediated by ATP.
For release of insulin, the beta cells of pancreas should be depolarised and insulin release is blocked when these cells are repolarised.
The release of insulin from beta cells of pancreas depends on the depolarisation/repolarisation state which is controlled by mediator like ATP. The elevated blood glucose is taken into the beta cells of pancreas which then undergoes glycolysis to release ATP. This ATP then blocks outward going potassium channels (which are highly sensitive to ATP) preventing hyperpolarisation. This can stimulate influx of calcium leading to depolarisation of beta cells releasing insulin.
Sulfonyl ureas
In type II diabetic patients, there may be insufficient release of insulin or even improper functioning of insulin. So in these patients glucose levels are persistently raised and more accumulated after a meal. Hence one of the approaches to control the blood glucose levels is to stimulate insulin release from beta cells of pancreas.
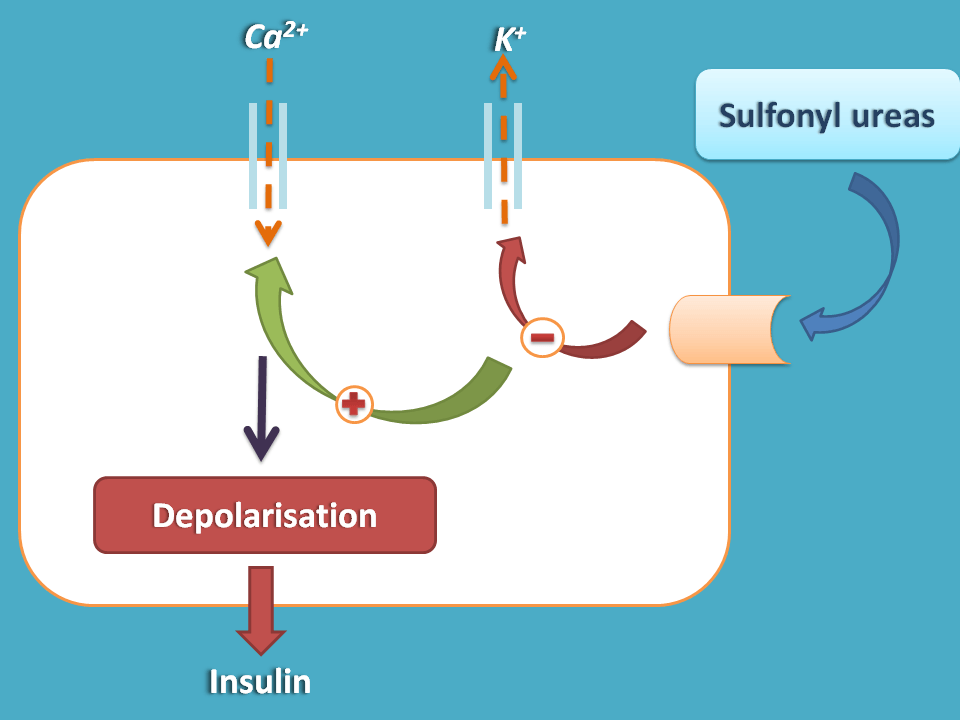
Sulfonyl ureas play a similar role like ATP and therefore block ATP sensitive potassium channels on beta cells. This inhibition of hyperpolarisation leads to depolarisation mediated by calcium influx and subsequent insulin release.
Since they act on B-cells to release insulin these drugs are also called as B-cell dependent insulin secretagogues.
Sulfonyl ureas can be divided in to two generations. Old generation sulfonyl ureas mainyl include
- Tolbutamide
- Chlorpropamide
Chlorpropamide is nowadays not used due to toxic effects.
New generation sulfonyl ureas are less toxic and more active. They include
- Glipizide
- Glyburide
- Glibenclamide
One of the main side effects of these drugs, obviously related to their main action, is hypoglycaemia.
Voltage gated chloride channels
Till now we have discussed drug targets acting either as blockers or activators. But we can find another class of drugs called benzodiazepines acting as positive allosteric modulators on GABA gated chloride channels.
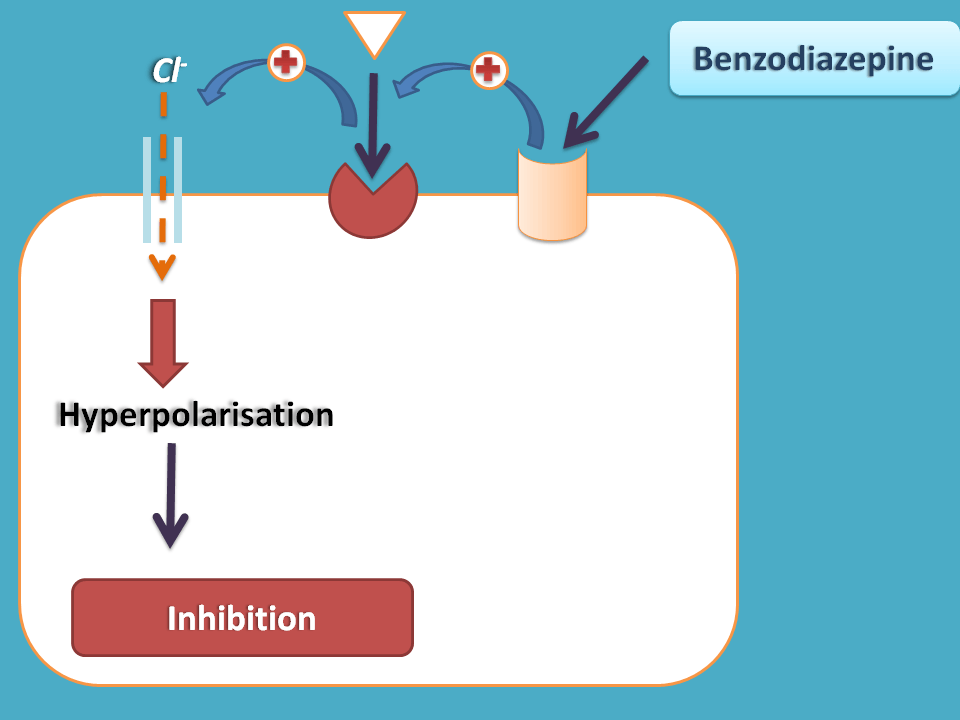
These drugs act at an allosteric site, which is a site other than the GABA binding site thereby produce a conformation al change at GABA binding site. This increases the binding of GABA on GABA binding site opens the inward going chloride channels leading to hyperpolarisation.
As the membrane is hyperpolarised any excitatory response like anxiety, aggressiveness and convulsions can be inhibited.
Various drugs included in this category are
- Diazepam
- Oxazepam
- Lorazepam
- Temazepam
- Halazepam
- Chlordiazepoxide
Few of the drugs like alprazolam, midazolam and triazolam are fused benzodiazepines with either triazole or imidazole.
All these drugs are safe in overdosage and less addictive compared with opioids. Hence these drugs are widely prescribed for acute anxiety disorders. Few of the drugs like lorazepam and triazolam can also be used as hypnotics to induce sleep.
So these are clinically very important and potential drug targets acting on potassium and chloride channels