What is the difference between repolarisation and hyperpolarisation?
by egpat Posted on 06-10-2017
Even both the process work in a similar fashion that they reduce membrane potential, a lot of difference exists between these processes. Both of these processes differ in their starting point and ending point.
What they do?
First let’s compare the roles of these two processes in physiological system.
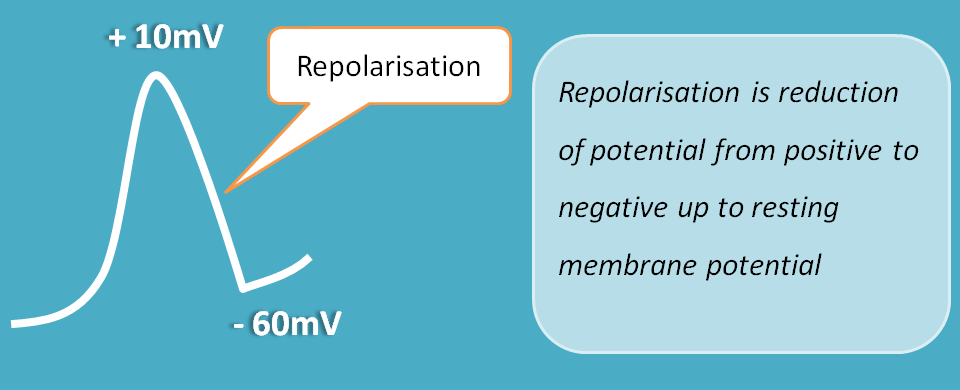
Repolarisation
Repolarisation is a reduction of the membrane potential from positive potential to negative potential up to the resting membrane potential. This brings the cell back to the resting state so that it can respond to the next action potential.
Repolarisation takes place in the cells which are already depolarized.
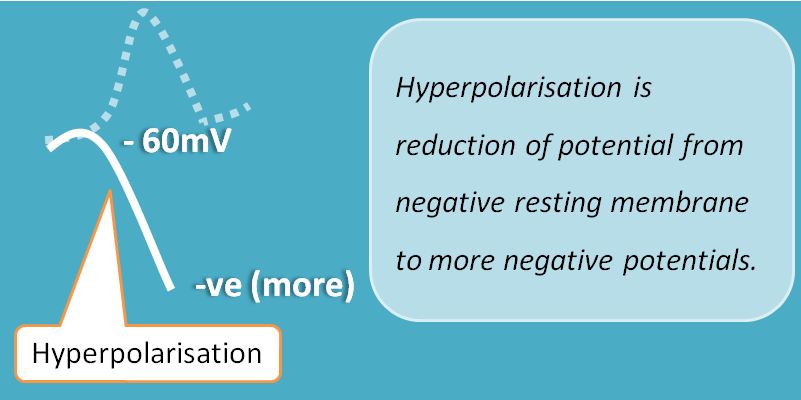
Hyperpolarisation
Hyperpolarisation is a reduction of potential from resting membrane potential to more negative potentials. This makes the cell less excitable even it receives action potential.
Hyperpolarisation takes place in the cells which are in resting state
How they operate?
We can also observe few differences and even similarities in how they produce their effects. So let's start with repolarisation.
Repolarisation
Repolarisation is a part of cellular process and it is essential. If repolarisation is inhibited, cell can’t be activated for the next time. So to maintain sustainability, repolarisation is required. Repolarisation is carried by outward going potassium channels in most of the cells.
Repolarisation is carried by outward going potassium
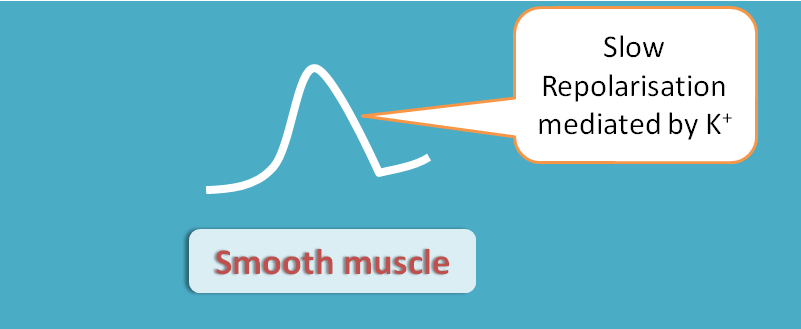
Repolarisation in smooth muscle is mediated by voltage gated potassium channels which slowly decrease the membrane potential to the resting membrane potential.
Just like smooth muscle, repolarisation in skeletal muscle also follows the same pattern by opening of voltage gated potassium channels, but somewhat fast compared to smooth muscle.
In contrast, repolarisation in cardiac muscle is prolonged. It shows two phases such as partial repolarisation phase and complete repolarisation phase. During partial phase a small current of outward potassium channels are opened leading to only a small reduction of membrane potential.
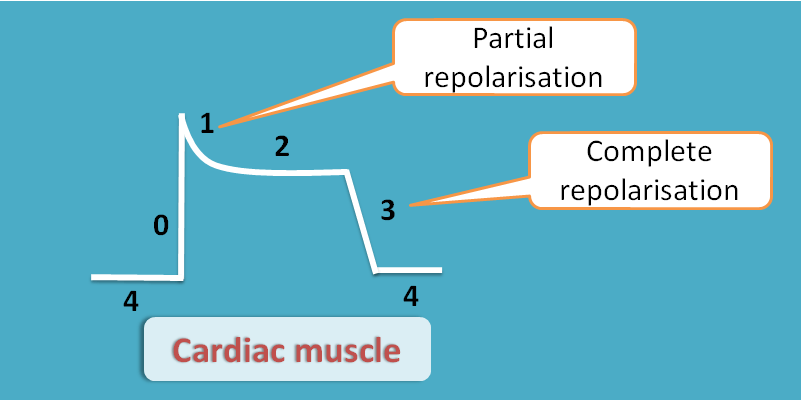
In complete repolarisation phase, a large potassium outflux brings the membrane potential back to the resting state so that cells are ready for next action potential.
Why two phases?
Cardiac muscle is a special type of muscle as it not only requires contraction and relaxation but also requires filling of blood into the ventricles. This can’t be achieved if repolarisation quickly follows depolarization. Therefore repolarisation is somewhat delayed by plateau phase during which adequate amount of blood can fill into the ventricles.
Drug targets
Class III antiarrhythmic agents like amiodarone, sotalol, dronedarone and mexiletine act on the repolarisation phase of heart and increase effective refractory period.
Hyperpolarisation
Hyperpolarisation is an inhibitory response so that the cells are in a state not to be responded by an action potential. The membrane potential is made quite negative than the resting membrane potential so that an action potential can’t open voltage gated sodium channels or calcium channels and bring depolarization. So the cell is in an inactive state not stimulated by action potential.
Hyperpolarisation can be mediated by either outward going potassium channels or inward going chloride channels. These potassium channels can be activated by mediators like acetylcholine or ATP. Similarly chloride channels are controlled by inhibitory mediator GABA.
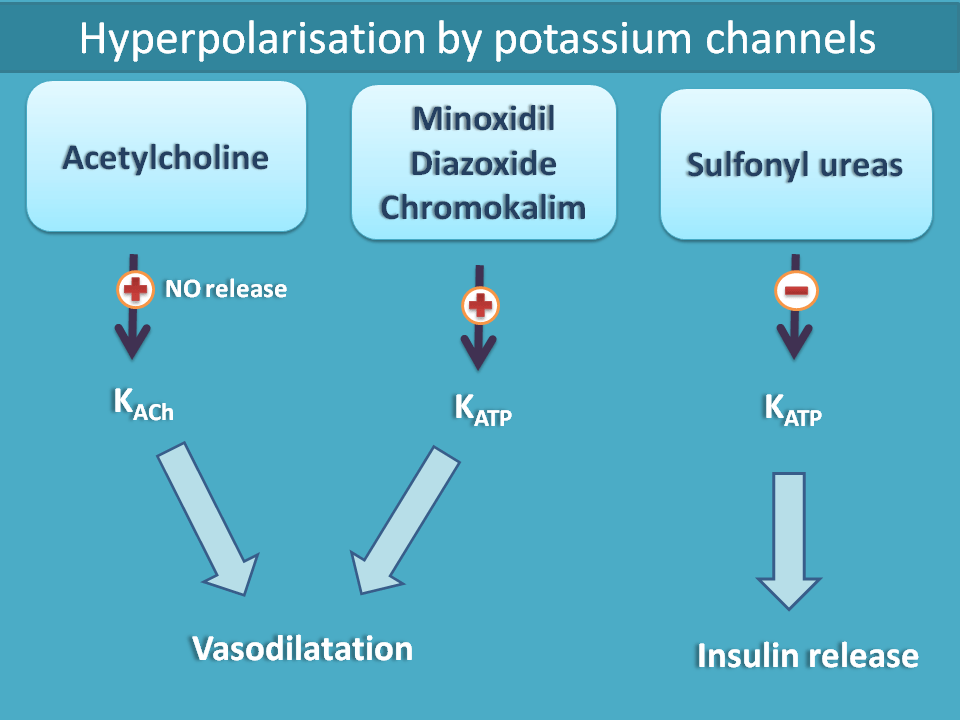
Parasympathetic mediator acetylcholine acts on vascular endothelium and releases nitric oxide. This released nitric oxide then opens potassium channels leading to hyperpolarisation. Similarly drugs like diazoxide, minoxidil, chromokalim and nicorandil all activate ATP-sensitive potassium channels leading to vasodilatation. On the other hand, sulfonyl ureas block ATP-sensitive potassium channels on beta cells of pancreas leading to depolarisation and release of insulin.
- For more details, see drug targets acting on potassium and chloride channels.
Benzodiazepines produce hyperpolarisation within the CNS by opening of chloride channels. These drugs act on GABAA receptors at allosteric site and increase the binding of GABA on GABA binding site.
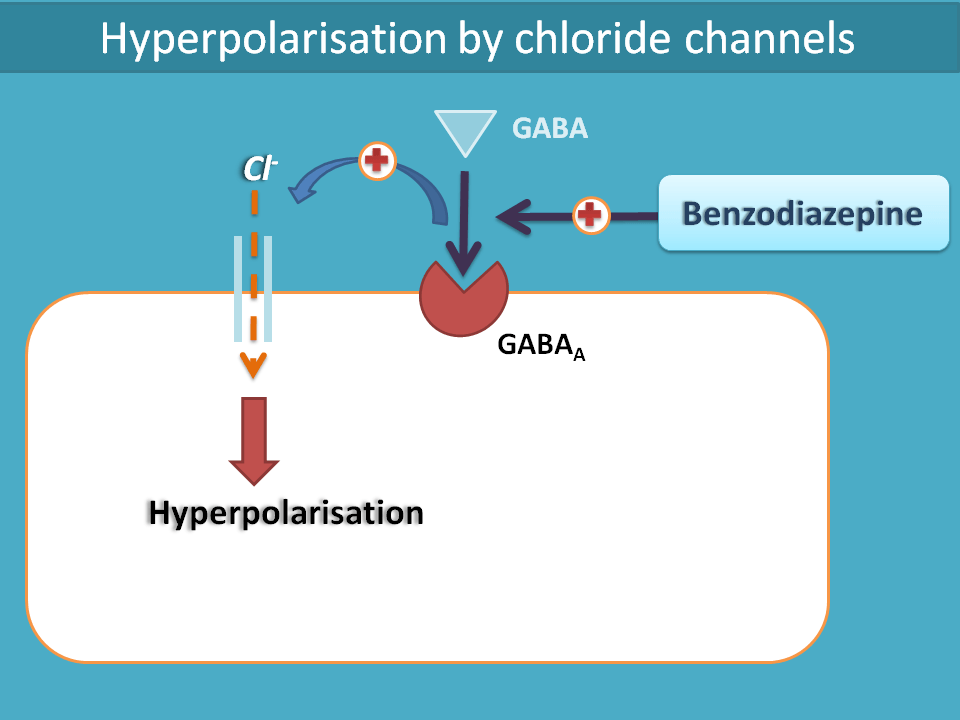
This opens the inward going chloride channels which influx into the membrane to produce more negative potentials. This hyperpolarisation causes inhibition of the target cells within the CNS resulting in decreased anxiety and aggressiveness in the patients. They also induce sleep and decrease the threshold for convulsions.
So finally we can conclude that repolarisation and hyperpolarisation are completely different process each having their unique roles in our physiological system.
Follow us
Join with us
Get the latest updates and posts
Follow us at