Non-selective alpha blockers
Non-selective alpha blockers have little clinical use today due to their adverse effects and non-selectivity in their actions.
Currently two drugs are included in this category such as
- phenoxybenzamine,
- phentolamine
Phenoxybenzamine
Phenoxybenzamine is a long acting non-selective alpha blocker. Chemically it is a phenoxyethyl benzamine with 2-chloroethyl substitution on nitrogen.
Why phenoxybenzamine is long acting?
One of the important structural moiety in phenoxybenzamine is 2-choloethylamino group which can form covalent bond with alpha receptors by removal of chlorine atom. Hence it produces irreversible block of alpha receptors and therefore long acting. It also blocks both uptake 1 and uptake2 process at adrenergic nerve terminals. But this may not be significantly related to its action.
Competitive or non-competitive?
As phenoxybenzamine produces irreversible block of alpha receptors, it can't be reversed by increasing the concentration of catechol amines hence it shows non-competitive antagonism.
One of the main use of phenoxybenzamine is to control the blood pressure by blocking alpha1 receptors thereby preventing action of catechol amines.
What is pheochromocytoma?
Why it is not used for regular treatment of blood pressure?
Even it decreases blood pressure by blocking alpha1 receptors, it is not completely selective for these receptors. It also acts on alpha2 receptors increasing norepinephrine release. Hence it produces pronounced side effects like reflex tachycardia.
Phentolamine
Phentolamine is another non-selective alpha blocker but short acting and reversible. You can remember the name from structural moieties. It has phenol group, toluene group and amine group. Hence it named as phentolamine.
Unlike phenoxybenzamine, it produces reversible block hence it is competitive.
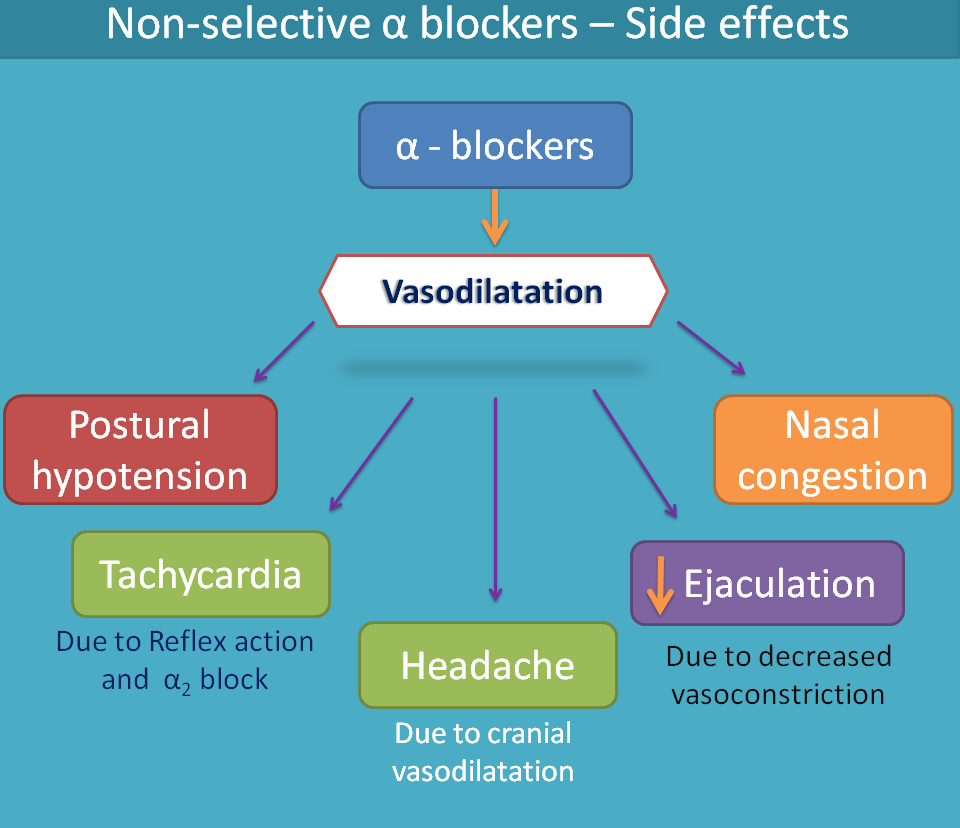
How they act?
Non-selective alpha blockers block both α1 and α2 receptors thereby produce mixed effects. By blocking α1 receptors they prevent action of catechol amines preventing activation of phospholipase C and release IP3 and DAG. AS these secondary messengers are not released, intracellular calcium levels in vascular smooth muscle are insufficient to produce contraction resulting in vasodilatation.
They also act on α2 receptors, which are presynaptic, and again inhibit action of catechol amines. But this time they increase norepinephrine release. As α2 receptors are autoinhibitory in nature when they are blocked the negative control on norepinephrine release is prevented enhancing the release of norepinephrine at synaptic cleft. In this way, they increase sympathetic discharge which then acts on beta receptors mainly on the heart. This results in to tachycardia.
You can easily observe that alpah1 blocker decreases adrenergic transmission whereas alpha2 bloke increases. But locations are different. The released norepinephrine by alpha2 blocker can mainly act on beta receptors as already alpha receptors are blocked by these drugs.
Follow us
Join with us
Get the latest updates and posts
Follow us at